Myeloproliferative Neoplasms (MPNs)
At present, the only curative option for Myeloproliferative Neoplasms, (MPNs), available in Australia is based upon one’s critical criteria, (symptom-burden, age, and their existing Quality of Life – QoL). However, that option, (an Allogenic Stem Cell Transplant – ASCT), which is usually only applied to those with advanced Myelofibrosis, (MF), or those who have progressed to Acute Myeloid Leukaemia, (AML), (and usually only when the patients are more senior in years), can often be too little, and far too late for many.
Research, followed by Clinical Trials, is where many new treatment drugs are tested, and not without some progress. From 2005 – 2013, three of the currently known ‘Driver’ mutations have been uncovered, and since that time new and more interesting potential treatments are slowly coming to light. However, much of this work is embryonic at this juncture.
In other nations overseas, where the medical fraternity believe in trying to prevent further progression by not waiting until MPN patients are too old to withstand the rigours of pre-stem cell transplant conditioning. Accordingly, and in some cases, they proceed much earlier to ASCT believing that being younger might benefit patients with far more positive outcomes. Graft Versus Host Disease (GVHD), is still a common problem for many who undergo this treatment, and results remain mixed at best.
Also in the pipeline, both here & overseas today, are many new, (and some previously tried treatments), reemerging in the hope of finding better ways to control MPN conditions by pursuing a range of different techniques, including:
- inhibiting genetic mutations in the MPNs
- CALR mutations may soon provide MPN patients w/ this mutation a monoclonal antibody
- preventing adverse impacts from stroke and blood clots
- reducing symptomatic effects
- earlier screening for adverse high-risk mutations
- Lobbying of governments to reduce the prohibitive costs of screening tests & pharmaceuticals
Hopefully, future research being undertaken here in Australia will soon see our our medical fraternity providing Australian patients with a greater range of treatment options also…
We also need to undertake more robust lobbying of our governments in the hope of reducing the costs associated with firstly diagnosis, prognosis, and with the cost of treatment options too…
Myelo, is a Greek term for bone marrow. Proliferative, refers to the reproduction process of excessively producing these cells through a process of cloning them, which may in turn cause an exponential abnormal production of, (Neoplasms or more simply), – new blood cells.
Our bodies, not unlike the process lines in any factory, produce a number of different types of blood cells. MPNs are conditions that are thought to be caused through abnormal cell mutations, that in turn, affect how blood cells are produced in our bodies. Generally speaking, it is believed that MPN mutations are acquired over the course of our life time rather than inherited genetic conditions.
Bone Marrow is the Place Where New Blood Cells Are Produced…
Genetic Mutations
There are generally speaking, two (2) types of genetic mutations that are referred to with an MPN diagnosis. The first type are called the ‘Driver’ mutations that also help in determining an MPN at diagnosis, and the second type are High-Risk (HR), mutations that might assist in understanding more about a patient’s prognosis, longevity, and overall survival.
Known ‘Driver’ MPN Mutation Types:
- JAK2V617F
- MPL
- CALR – Types 1 & 2
- Triple negative
- Unclassifiable
It’s now known that many MPNs are related to genetic mutations, and a protein in our bodies called JAK2. JAK2 is a protein which regulates blood cell production. It is common for anyone with an MPN to show a mutation in the JAK2 protein. JAK2 mutations were only uncovered in circa 2005. Shortly thereafter, other mutations were also discovered such as MPL, (2005-6), and CALR, (2013).
The common factor to all these mutations is that they make the JAK2 protein overactive. Generally, these mutations occur in adulthood, hence, people are usually not thought to be born with them but rather that they acquire them during their lives.
Anne Mullally (MD), presents a short video below, which explains more about the three (3) most common known ‘Driver Mutations’ and how the CALR mutation might hold some future promise for a cure…
Other High-Risk (HR) Mutations
There are some other known HR genetic mutations that can also have a variety of adverse impacts upon a patients MPN condition depending upon their age, and possibly many other variables. Sometimes, even the order that these mutation appear in, (before or after the driver mutations), which is not always easy to determine without proper screening done via laboratory mutation panel testing.
In Australia, it is often an expensive exercise to ascertain these types of tests, and at the present moment they are only available from a restrictively limited number of medical institutions. It is often by knowing the order of those mutations that further prognosis might become available to a patient. Some of those high risk mutations might include any of the following:
- ASXL1
- EZH2
- IDH1/2
- SRSF2
- TET2
- TP53
Blood cell chronology
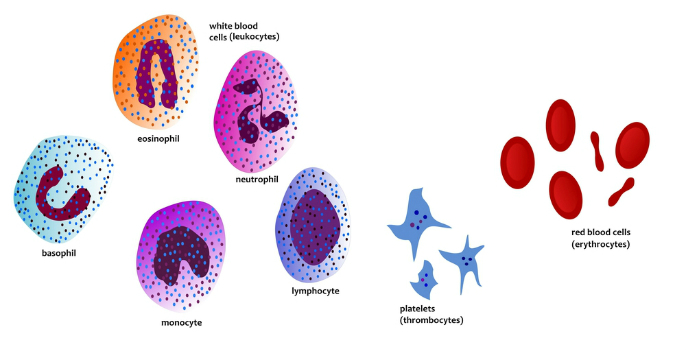
Essentially, the human body’s bone marrow produces three (3) types of Blood cell:
Red Blood cells (erythrocytes), Blood Platelets (thrombocytes), and White Blood cells (leukocytes).
There are three (3) classical types of MPN, (although there a few other less common types too), and each type of cell has a slightly different disorder attached to its diagnosis although symptoms can and often are very similar in effect on the patient.